The following discussion contains excerpts of the following notes, based on the 2nd Philippine edition of Nies and McEwen’s Community and Public Health Nursing (Famorca) textbook, as well as supplemental information by the lecturer. There are a lot of topics under Epidemiology and FHSIS that were not covered, so I recommend give those a read. Family also contains the Home Visit and Bag Technique topics, which are also key topics for the CHN board exams (apparently).
As discussed by Ma’am Aida V. Garcia, RN, MAN
Demography
The study of the population, entailing not only the size, but the composition and distribution as well. Some sources of demographic data include:
- Census: either de jure (actual residence), or de facto (based on where the individual is currently situated) performed by the National Government. It is the most expensive form of data collection in terms of both money and time (done every 5 years).
- Registration System: records of vital events e.g. birth certificate, death certificate
- Births should be reported within 30 days by the birth attendant or who birthed the child to the local civil registry.
- Deaths. In terms of location to register, this should be done where the death had occurred. The certificate should be signed by the municipal health officer.
- Sample Survey: selecting a small subset of the community in order to represent the entire community.
Population Size
In the Philippines, the global population is increasing by 1.6% (2020). In general, this change is based on absolute increase; calculated by deducting deaths from births. The same represented in percentage is called the relative increase.
- The age group with the most births is the 25 to 29 year old bracket of women.
- The total fertility rate includes all women from 15 to 49 years old who are still within the reproductive age. As of 2022, the amount of children per woman is 1.9.
- Crude Birth Rate (CBR) is the rate of births. The inversion is Crude Death Rate (CDR), the rate of death. The rate of natural increase is .
- The most common cause of mortality is lifestyle; the most common cause of morbidity is infection.
The population may also be described based on its composition, a primary example being of its gender. This is calculated with the sex ratio:
Composition may also be represented by age. The median age denotes the middle point of age in the population. Others include:
- The Dependency Ratio: the number of people who are economically dependent (unemployed, not employable; 0 to 14 years old, 65 years old and above) or economically independent (able to work; 15 to 64 years old).
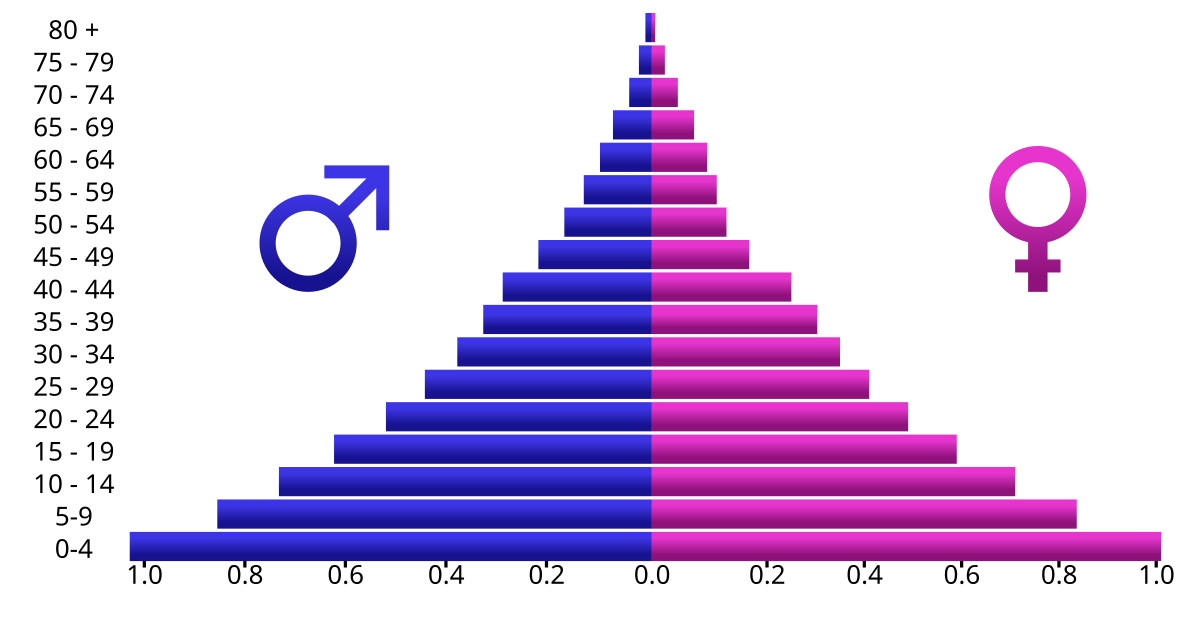
The representation of both age and sex with one graph utilizes the population pyramid graph.
The geographical and housing distribution of the population can be quantified through the following:
- Urban-Rural Distribution: the distribution of the population between urban and rural areas.
- Crowding Index: number of individuals per room in a household. Exceeding two indicates increased risk, especially for communicable diseases.
- Population Density: number of individuals within a given area (per km²).
Field Health Services and Information System (FHSIS)
A Health Information System (HIS) has four primary functions: data generation, compilation, analysis & synthesis, and communication & use. This system collects data from the healthcare and other pertinent sectors; analyzes gathered data; ensures overall data quality, relevance, and timeliness; and, converts the data into information imperative for health-related decision-making (WHO, 2008b).
The Field Health Services Information System (FHSIS) is the HIS utilized in the Philippine context, serving as the official reporting and recording system of the Philippine Department of Health (DOH). It is a facility-based and data-generated system from the Barangay Health Stations (BHS) and Rural Health Units (RHU) to the national level. The current FHSIS (version 2012) primarily aims to:
- Provide raw and summary data on health service delivery and selected health program accomplishment indicators;
- Provide a standardized, facility-level data base for program monitoring and evaluation purposes.
- Provide more evidence-based data for research purposes, policy formation and basis for health system interventions; and
- Minimize documentation burden at the service delivery level in order to allow more time for patient care and health promotion activities.
Components of the FHSIS
There are two primary types of tools utilized by the FHSIS:
- Recording Tools: detailed, day-to-day, facility-based documents on the health services rendered to patients/clients in the rural health facilities.
- Reporting Tools/Forms: summary data transmitted or submitted on a monthly, quarterly, and annual basis to higher organizational levels of the healthcare delivery system. These are based on the Summary Table (ST) and Monthly Consolidation Table (MCT) recording tools.
Recording Tools
- Individual Treatment Record (ITR): the primary building block of the FHSIS. This is a basic patient consultation record containing a date, name, address of the patient, height, weight, chief complaint, presenting signs and symptoms, diagnosis (if available), and treatment. Examples of ITRs include immunization records or national tuberculosis program treatment record.
- Target Client List (TCL): the secondary building block of the FHSIS. This is a list of eligible clients for a particular health program. It facilitates the monitoring and supervision of service delivery activities and determines the client’s compliance to a particular program. Health programs to be maintained under FHSIS version 2012 are: Prenatal Care, Post-Partum Care, Nutrition and Expanded Program for Immunization, Family Planning, and Sick Children. This tool provides a clinic-level data for population-based research.
- Summary Table (ST): a form with 12 columns for a monthly tally of the number of clients in the barangay health facility in terms of health program accomplishments (all TCL data) and morbidity diseases.
- Monthly Consolidation Table (MCT): a form filled up by the Public Health Nurse (PHN) to collate data report by all midwives of the city or municipality. It is essentially the output table of the RHU, consisting of the reported data per indicator by each Barangay Health Station or public health midwife. This record will serve as the source document for the public health nurse for the Quarterly Forms.
Reporting Forms
It will be important to memorize each report’s alias!
- Monthly Forms:
- Program Report (M1) contains selected indicators categorized as maternal care, childcare, family planning, and disease control; the same indicators found in the TCL and ST. This is report is submitted by the midwife.
- Morbidity Report (M2) contains a list of all diseases by age and sex. This report is submitted by the midwife.
- Quarterly Forms:
- Program Report (Q1)
- Morbidity Report (Q2)
- Annual Forms:
- Report on demographic, environmental, natality, and mortality. (A1)
- Report on all diseases according to age and sex. (A2)
- Report on all mortality cases or deaths according to age and sex. (A3)
Summary of Responsible Persons and Schedules for FHSIS Tools
| Office | Person | Recording Tools | Reporting Tools | Schedule |
|---|---|---|---|---|
| BHS | Midwife | ITR, TCL, ST | M1, M2 | Every second week of the succeeding month |
| - | A-BRGY Form | Every second week of January | ||
| RHLI | PHN | ST, MCT | Q1, Q2 | Every third week of first month of succeeding quarter |
| A1, A2, A3 | Every third week of January | |||
| PHOiCHO | Prov/City FHSIS Coordinator | - | Q1, Q2 | Every fourth week of first month of succeeding quarter |
| A1, A2, A3 | Every fourth week of January | |||
| CHD | Regional FHSIS Coordinator | - | Q1, Q2 | Every second week of second month of succeeding quarter |
| A1, A2, A3 | Every second week of March | |||
Family
There are many definitions of the family:
- The family is a group of persons usually living together and composed of the head and other persons related to the head by blood, marriage or adoption. It includes both the nuclear and extended family. (National Statistical Coordination Board)
- A social unit interacting with the large society. (Johnson, sociologist)
- A family is characterized by people together because of birth, marriage, adoption, or choice (Allen et al.).
- The family is composed of two or more persons who are joined together by bonds of sharing and emotional closeness and who identify themselves as being part of the family. (Friedman et al.).
The family is considered as a “unit of service” for the following reasons:
- The family is considered as the “natural” and fundamental unit of society.
- The family as a group generates, prevents, tolerates, and corrects health problems within its membership; the family acts as the basic care provider.
- The health problems of the family are interlocking. Illness in one member affects the entire family and its functioning.
- The family is the most frequent focus of health decisions and actions in personal care.
- The family is an effective and available channel for nursing efforts. Improved community health is realized only through improved family health.
Family Structure
| Family Form | Description |
|---|---|
| Nuclear | ”Traditional; Family of marriage, parenthood, or procreation”. A husband, wife, and their children— natural, adopted, or both (Friedman et al.). |
| Dyad | ”Empty nesters”. A husband and wife with no children. |
| Extended | ”Multigenerational”. Three or more generations, which may include in-laws and grandparents. |
| Blended | The union of two spouses who have had children from a previous marriage. |
| Compound | A husband with multiple wives, primarily only permitted in Muslim culture (in the Philippines) by virtue of P.D. No. 1083 (Code of Muslim Personal Laws of the Philippines). |
| Cohabiting | ”Live-in”. An unmarried couple and their child or children, recognized through common-law marriage. |
| Single Parent | Resulting from death of a spouse, separation, or pregnancy outside of wedlock. These families are faced with greater risk associated with lesser social, emotional, and financial resources. Families who have one of the spouses working overseas effectively fall under this category. |
| Homosexual | A cohabiting couple of the same sex in a sexual relationship. They may or may not have children. E.O. 209 (Family Code of the Philippines) expressly states that marriage is between a man and a woman, therefore disallowing same-sex marriage. |
| The following are additional forms and classifications discussed but not included within the book. |
Based on Authority, where decision-making is delegated to either the father (Patriarchal) or mother (Matriarchal). A participative form of authority is termed Patricentric, Matricentric or Egalitarian (equal), eliminating the hierarchal nuance of previous terminology.
Based on Marital Residence Pattern, where the family moves closer to or at the father’s residence (Patrilocal), moves closer to or at the mother’s residence (Matrilocal), or independent of either spouse’s location (Neo-Local)
Based on Lineage; the system of descent and inheritance where lineage, family name, and property are passed down the male line (Patrilineal) or the female line (Matrilineal)
Based on Amount of Partners, a family may be Monogamous, where one husband is bound to one wife; Polygamous, where a husband is with multiple wives (commonly found among Muslims in Saudi Arabia); or Polyandrous, where a wife is with multiple husbands (commonly found in the Todas of Southern India).
Functions of the Family
- Procreation: the universally accepted institution for reproductive function and child rearing.
- Socialization of Family Members: the family creates the foundation for how its children becomes productive members of society. It involves the transmission of culture from the parents to their children.
- Physical Maintenance: the provision of basic needs for its dependent members.
- Economic Function: the family serves as a basic unit of economic production (rural families producing goods) or economic consumption (urban families earning salaries or wages)
- Welfare and Protection: the family provides companionship and meets affective, sexual, socioeconomic needs, and emotional gratification. The family is a source of motivation and morale for its members.
- Status Placement: the family confers its societal rank on the children. With social mobility, the family may shift between social classes.
Family as a Client
The family unit is important to society. It meets individual needs, and supports spouses or partners by meeting affective, sexual, and socioeconomic needs. The family is also viewed as an important unit of health care with awareness that the individual can be best understood within the social context of the family. Observing and inquiring about family interaction enables the nurse in the community to assess the influence of family members on each other. Specifically, reasons to work with families are enumerated by Friedman et al.:
- “The family is a critical resource”; the family can improve individual members’ health through health promotion and wellness activities.
- “In a family unit, any dysfunction that affects one or more family members will affect the members and unit as a whole”; this is also referred to as a “ripple effect”.
- “Case finding”; while assessing an individual, the nurse may identify a health problem that necessitates identifying risks for the entire family.
- “Improving nursing care”; the nurse provides better and more holistic care by understanding the family and its members.
The family as a system
The General Systems Theory explains how the family as a unit interacts with larger units outside the family. There are three subsystems of the family that are most important: parent-child subsystem, marital subsystem, and sibling-sibling subsystem. Each subsystem can reestablish balance if any disrupting force or imbalance occurs.
Developmental Stages of the Family
Like with the growth and development of pediatrics for individuals, families also experience stages of development traversing from marriage to death. The nurse must comprehend these phases and the struggles that families experience while going through them. Developmental tasks exist for these stages, and are the resolution to each stage.
- Marriage (joining of families): the formation of an identity as a couple, and inclusion of the spouse in realignment of relationships with extended families.
- Families with young children (to age 12): problems arise with who is to take care of the children; the integration of children into the family unit, adjustment of tasks for child-reading, financial, and household; accommodation of new parenting and grandparenting roles.
- Families with adolescents: development of increasing autonomy for adolescents; midlife reexamination of marital and career issues. This is the initial shift towards concern for the older generation.
- Families as launching centers: establishment of independent identities for parents and grown children; renegotiation of marital relationship, readjustment of relationships to include in-laws of older generations
- Aging families: maintaining couple and individual functioning while adapting to the aging process, supporting role of the middle generation, supporting and autonomy of the older generation, and the preparation for their own death and dealing with the loss of spouse and/or siblings and other peers.
Health Tasks and Characteristics of a Health Family
The family serves as an essential resource for its members by carrying out health tasks. An important responsibility of the community health nurse is to develop the family’s capability in performing its health tasks (Freeman, Heinrich):
- Recognizing interruptions of health or development: a requisite step to dealing with an unacceptable health condition.
- Seeking health care: consultation with health workers if the health needs are beyond its capability.
- Managing health and non-health crises: maturational (foreseeable) and incidental (unexpected) crises that require coping and adaptation.
- Providing nursing care to sick, disabled, or dependent members of the family: many minor illnesses, chronic conditions, disabilities, and some age groups require home management by responsible family members.
- Maintaining a home environment conducive to good health and personal development: a safe and healthful physical environment, and an atmosphere of security and comfort for psychosocial development.
- Maintaining a reciprocal relationship with the community and its health institutions: just as the family utilizes community resources, the family also gets involved in community events.
Otto (1973) and Pratt (1976) characterized health families as “energized families” and provided descriptions of healthy families to guide in assessing strengths and coping. DeFrain (1999) and Montalvo (2004) helped to identify health families. They suggest the following traits of a healthy family:
- Able to communicate and listen repeatedly in many contexts
- Able to establish priorities and family needs
- Affirms, supports, and respects each other
- Members engage in flexible role relationships, share power, respond to change, support growth and autonomy, and decision-making
- Teaches family and societal values and beliefs, sharing a spiritual core
- Fostering responsibility and values service to others
- Has a sense of play and humor and shares leisure time
- Able to cope with stress and crisis and grow from problems